I have an affinity for weird-looking plants and animals. Moose? I love their big, fat noses and crazy antlers (although they’re also terrifying when you see one close-up!). Penguins, their amusing waddling. Walruses: their hysterical mustaches, although, again, terrifying up close. hahaha.
And there are so many amazing, weird plants out there.
One such weird, fascinating plant is the Utah Juniper Tree.
A juniper tree at “Hell’s Half Acre” near Blackfoot, Idaho.
When I lived in Southeast Idaho, I spent a lot of time driving between there and everywhere else, including Utah and California. Near Blackfoot, Idaho, there is a large volcanic scar that runs along the highway for a time. I love the look of the green or brown (depending on the season) grass and other plants against the black rock. But I was always fascinated by the gnarled trees that jut out at odd angles straight from the rock, even on cliff faces. I wondered how the trees survive. I couldn’t see any kind of soil. There’s a rest stop that has some walking trails and I stopped once to check it out and discovered the trees are Utah Junipers. They are native throughout Southern Idaho, Colorado, Northern Idaho and some parts of Southern California–but mostly found in Utah.
They’re the trees of the high desert.
Not much can survive the arid, harsh conditions of the high desert–yet, here, the Utah Juniper thrives. It grows slowly, so slowly. A tree can be hundreds of years old, but less than 25 feet tall. But its height, or lack thereof, is not what makes it interesting to me.
The wind whips and whirls almost constantly along the rocky, dry earth, shaping the juniper trees into gnarled, twisted, and distinctive formations. Yet, the perpetually blowing wind of the Western Desert does not destroy the tree. It hardens it, weathers it, and shapes it. The experiences of the Utah Juniper’s life make it unique, beautiful, and strong.
Life in the high desert is not easy for plants. Such arid conditions leave the rocky surface riddled with dead, dried grasses–remnants of a spring thaw long past. Most plants burn up and wither away within one season. And yet, here lies the Juniper tree surviving–thriving even–slowly building itself up year after year, inch after inch, to reach its full potential sometimes for 750 years or longer. Giving itself the grace to grow whatever it can grow, however it can grow, with the resources it has.
Its roots grow stronger and deeper each year as it finds nourishment in the rocky ground in which it grows. A tree may be 15 feet tall, but the main tap roots can be 40 feet deep into the rock, with lateral roots growing out 100 feet away from the tree. The root system often accounts for 2/3 of the total tree mass. Because the roots are so hardy, even when the wind knocks the tree over, it will continue to grow. No matter the intensity of the burdens of the weather, it continues to cling to the sides of mountains, to cliffs, to life, and keeps growing. They are patient in their perseverance.
The tree also sustains life around it, providing food and shelter for birds and small animals. It takes the harshness of the environment and turns it into something life-giving for all those around it.
These fascinating trees and their determination to cling to life make me feel so hopeful.
“Hope in a gospel sense is hope in Christ. And hope in Christ simply means that we trust Him and we trust in our Heavenly Father’s plan.”
“Therefore, hope is expectation, even anticipation for happiness not only in the hereafter, but an expectation that we can have joy and contentment right now, regardless of our circumstances.”
She continued, “Waiting can mean being stifled, biding one’s time, or stopping. “But to ‘wait upon the Lord’ is not biding one’s time. It is being patient while moving forward with confidence, faith, and trust in the Lord’s plan for us.”
The Lord, at times, gives personalized and tailor-made challenges designed to help His children grow.”
“Hope, on the other hand, is like the beam of sunlight rising up and above the horizon of our present circumstances. It pierces the darkness with a brilliant dawn. It encourages and inspires us to place our trust in the loving care of an eternal Heavenly Father, who has prepared a way for those who seek for eternal truth in a world of relativism, confusion, and of fear….
Hope is not knowledge,17 but rather the abiding trust that the Lord will fulfill His promise to us. It is confidence that if we live according to God’s laws and the words of His prophets now, we will receive desired blessings in the future.18 It is believing and expecting that our prayers will be answered. It is manifest in confidence, optimism, enthusiasm, and patient perseverance.”
The things we hope for are often future events. … No matter how bleak the chapter of our lives may look today, because of the life and sacrifice of Jesus Christ, we may hope and be assured that the ending of the book of our lives will exceed our grandest expectations. …
The things we hope in sustain us during our daily walk. They uphold us through trials, temptations, and sorrow. Everyone has experienced discouragement and difficulty. Indeed, there are times when the darkness may seem unbearable. It is in these times that the divine principles of the restored gospel we hope in can uphold us and carry us until, once again, we walk in the light.
We hope in Jesus the Christ, in the goodness of God, in the manifestations of the Holy Spirit, in the knowledge that prayers are heard and answered. Because God has been faithful and kept His promises in the past, we can hope with confidence that God will keep His promises to us in the present and in the future…
The things we hope for lead us to faith, while the things we hope in lead us to charity. The three qualities—faith, hope, and charity35—working together, grounded on the truth and light of the restored gospel of Jesus Christ, lead us to abound in good works.36
With Nephi I declare: “Press forward with a steadfastness in Christ, having a perfect brightness of hope, and a love of God and of all men. Wherefore, if ye shall press forward, feasting upon the word of Christ, and endure to the end, behold, thus saith the Father: Ye shall have eternal life.”39
If the trees were sentient, they may wish they didn’t live in such a windy and severe climate. But then they wouldn’t have such an interesting and unique look. The wood would not be hardened and useful to the people who lived in these locations for centuries, who used it as firewood and fencing. They wouldn’t be able to give shelter, nutrients and protection for the surrounding area for centuries.
May we not be like the single-season grasses but rather the Juniper tree that sends its roots out deep and wide and provides shelter and nourishment to those all around it. May we find peace and hope we continue to persevere through winds that beat at us and dig as deep as we need through the dry desert sands at our feet to the eternal well of the Savior’s Atoning Waters.
This might be my favorite project I’ve made to date. I saw an incredible flower headpiece photo online and knew I wanted to make something inspired by it for an office St. Patrick’s Day lunch. We were supposed to wear our most outrageous outfits. I wasn’t feeling outrageous, but I was feeling big—as in a big hat. Haha.
Making the Hat Base
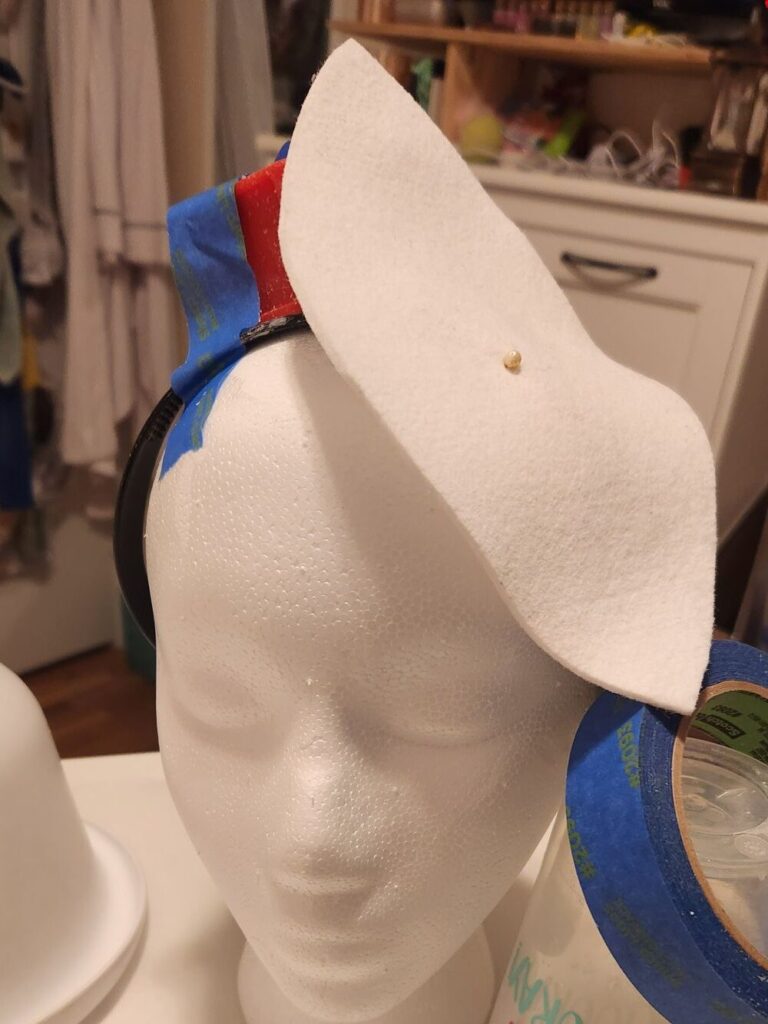
I had made a small fascinator a few years ago. It’s a small, cute pink and white one. But this needed to be big. Statement making. Over the top, perhaps? lol. I wanted it to angle over my eye and go up in the back. So I needed to figure out how to make that happen. I found some tutorials online and realized that I needed fabric stiffener. I drew up a rounded diamond-ish shape I liked and then soaked it in stiffener, shaped it, and left it overnight to dry. Surprisingly it worked! I then added a “loop” underneath so a headband can slip through and hold the hat in place. It mostly worked. It ended up being a little heavy for the style of headband I wore.
Rigging up a solution to shape the felt base the way I wanted while the stiffener dried. It worked!Shaping the hat worked!
Creating the Flowers
Then I got to work on flowers. I loved the huge orchids on the inspo photo so I made three big ones, with some flower buds up at the top so it looked more like a branch. I used the branch as the basic armature of the hat. There needed to be some accent flowers. Since this was for a St. Patrick’s Day party, I went with seven gold roses.
The paper orchid branch and roses are ready to be added to the hat base. I ended up making another small rose to tuck into an empty spot.
The full-sized orchids are about six inches across—they are big! The biggest rose is about five inches and gets progressively smaller.
Testing out rose placement.Here, you can see how the headband slips through a “loop” underneath the hat base.
Making the Leaves
Once I had the roses added, I knew I needed some greenery. Maybe lots of greenery?
Green crepe has a bad habit of fading and bleaching out in the sun, so I was hesitant to use it for this project, because I wanted it to have longevity. There are sprays that can be used to help with color fixing, but they are not permanent. One way to help combat this is to paint or dye your own crepe. I chose to do this for my green. I’ve painted green crepe for my rose leaves before. This time, I wanted to try dyeing white crepe green. I picked up acrylic ink in a variety of blues, yellows, and greens (even a silvery green, which gave the leaves a cool, subtle shimmer). If you are looking for these paints, I suggest looking at Michaels and when they are on sale or if you have a coupon.
I decided on a leaf shape roughly similar to a blue gum eucalyptus (my favorite!) and cut my white crepe paper into strips that would be that leaf length. I mixed the paint with water and put the paper strips in to absorb the color. Then, I went back over the paper with additional drops of paint as it was drying but still damp to get more color variation. I LOVE HOW IT TURNED OUT. I will definitely be doing this method again. The color was amazing.
Drying dyed paper on cookie sheets. These will become the leaves. I love how the variegation turned out on the leaves!
Adding the Greenery
Leaves added to the back of the hat.
I glued the leaves individually to the armature so I could place and shape them where I wanted. The nice thing about having wired leaves (and petals, if the flower calls for it) is that you can shape the leaf and have it go wherever you like. It was fun to have the leaves curl, bend, and weave throughout this project.
I needed “ground cover” in a blank spot in the back, so since it was St. Patrick’s Day, I added tons of little clovers. I used the template I put together from my redwood sorrel (which isn’t related). There is a four-leaf clover in the clover patch. It’s hiding in the back a little, towards the bottom (not really visible in the photo below).
Clovers having their moment in the back of my orchid hat. I added a little bling and sparkle to give it my “extra” signature. haha.
Finishing Touches
Next were the finishing touches. Adding the leaves, the green wire loops I’d made, and feathers I’d picked up at a local craft store.
Testing out the placement of the wire loops and feathers I made.
The wire loops were 20 gauge wire wrapped in green crepe paper. I made 15 lengths and grouped them into five groups of three. Then, I wove them in and out of the flowers and leaves.
I found an ostrich feather “branch” at a craft store and loved it so much I just had to incorporate it. There are two sections at the top and one at the bottom. With these added, the hat is 24 inches long! I did make them removable. lol.
It needed something else. Some pièce de résistance. I had already added a touch of glitter in the back and didn’t want to add more. But gold leaf? YES. I added patches of it in random spots all over. I loved how it turned out.
Gold leaf added randomly to the leaves and petals.
Gold leaf added randomly to the leaves and petals.
Gold leaf added randomly to the leaves and petals.
So sparkly in the restroom light! lol
Finale
If you’ve made it this far, bravo! Let’s see how it turned out!
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Finished Orchid and Rose Fascinator DIY
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Orchid and Rose Fascinator
Orchid and Rose Fascinator
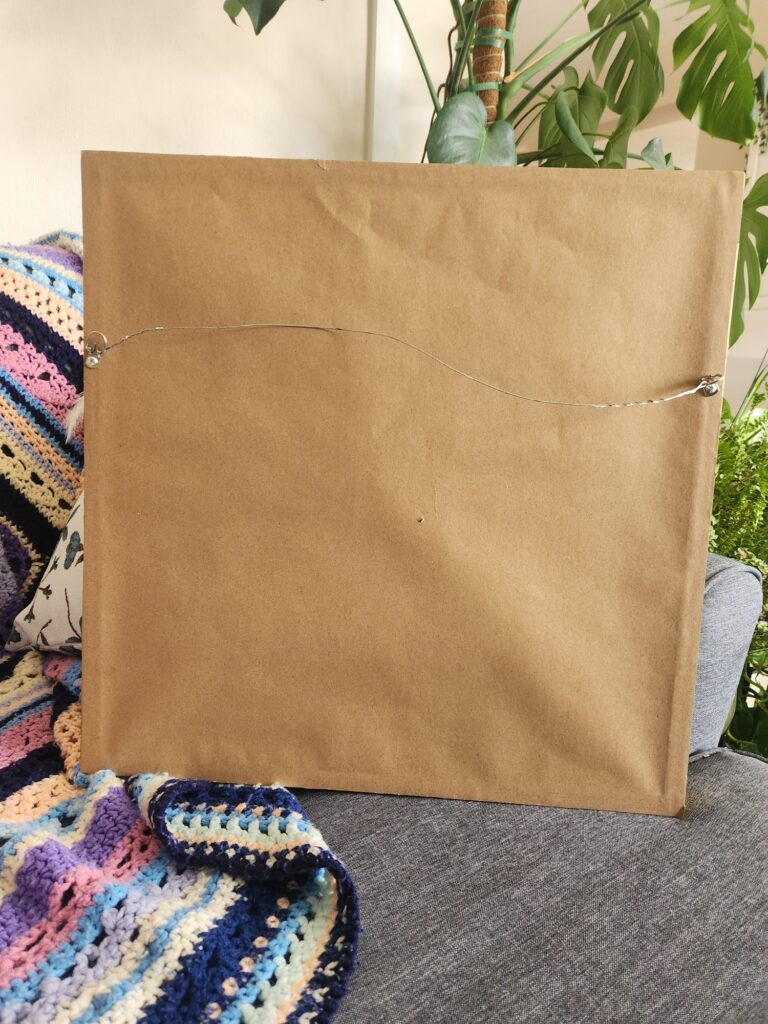
After it was a hit at the party (if I do say so myself, lol), I needed a way to store it safely. I found a large frame at a thrift store and thought it was perfect for mounting the fascinator. I refinished the gold with some rub ‘n’ buff. Then, I mounted the hat on cardstock. I used zip ties to attach it to the frame so I could clip it out if I wanted to use the hat again. I’m pretty proud of how professional it ended up looking!
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
Mounted and framed Orchid and Rose Fascinator
To wrap up this post, I entered it at the State Fair this year and got a First Place Ribbon!
I got normal lab results again recently. It was just a CBC with differential. Nothing big. But still another poke. I’m used to labs by now. I can tell the phlebotomist exactly where to poke me for the best access (the back of my hands, towards the outside). “And when it likely fails, don’t worry, new friend, it’s me, not you,” I say every time. They inevitably laugh and say they’ll be able to get it because the vein looks excellent. Their naivety is adorable. I smile tightly. “Yep. it sure does.” And sigh on the inside. I have terrible veins that don’t like to cooperate. Drawing blood is much easier than setting an IV, though. IVs often take multiple attempts and multiple nurses. This time, I was lucky, and the phlebotomist got me on the first poke. I still have a nice hematoma, though.
The results came back the next day. I am the picture of health according to them.
Ha. Ha haha hahahahahahahahaha. Excuse me while I try not to have an asthma attack from laughing so hard.
Clearly, I am not.
But yet, that is what my labs almost always say—normal results. All my tested biomarker levels are in healthy ranges. Well, that’s just great. I’m glad they are. Really, I am. It means my medication isn’t damaging my organs (yet), and my immune system is managing to be okay. But that doesn’t help us measure what is happening in my body.
The labs, of course, provided no real answers—except what was not wrong with me. This is helpful to an extent—don’t get me wrong—but ruling things out is almost as helpful—but they are not the actual answers.
Labs
The problem with my condition is that very few labs can actually measure what is going on. And those few labs are notoriously tricky to do. The chemicals measured are extraordinarily fickle and break down very quickly. Sample collection requires collecting urine in a particular container for 24 hours and keeping it chilled the entire time. The samples have to be constantly refrigerated, even during transportation. Even 5 minutes outside of a cooler can ruin the 24 hours of work (and it is work!). There’s a bit of art in keeping the samples chilled. Patient groups frequently pass these tips on to the “newbies.”
Few laboratories are equipped to perform the labs, and fewer are knowledgeable enough to keep everything adequately chilled. The margin for error for these tests is massive, and they are unreliable. A negative result doesn’t rule out anything. It probably means someone messed up the test. Even when everything is supposedly done properly, results can be inconclusive or normal. It’s incredibly frustrating—all that work and expense for naught. Many patients try these labs repeatedly, trying to get the elusive positive result.
When I was first diagnosed in 2015, I had more labs that came back unhelpful. I did everything right, but I still didn’t get ideal lab results that conclusively proved my diagnosis. Fortunately, my doctor felt (and others have since agreed) that the labs and my symptoms were enough to give me my diagnosis. I am so, so grateful. Not every patient is so lucky.
When I got sick at age 14, I learned the anguish of labs that don’t provide answers. I remember one phlebotomy session where 18 large vials of blood were taken. Then, I had a bleeding time test. They were trying to figure out if I had a clotting disorder, among many other things, I’m sure. I remember thinking that it was ironic they were taking so much blood when we had just had a conversation with the doctor about whether I needed a blood transfusion because of how little blood I had. I do have a blood disorder–they were right about that, but the fickle labs for it wouldn’t be invented for another 10+ years. My condition wouldn’t even have a name for another 10 years. It was impossible to find then.
Countless labs have followed in the years since. More normal or inconclusive lab results. Maybe this time will be when my body finally objectively proves something is wrong? No, not this time.
But I am sick! I yell at the screen of normal numbers. Why won’t you show that!? Something is wrong. Please show the doctors I am not making this up! Please tell them I am not crazy! For once. just tell us something helpful. Please!
Objective vs. Subjective Findings
Doctors like to have something to show them what’s wrong, something to justify the symptoms. They like to measure and count, which allows them to mark improvement or digression. When labs don’t support the patient’s symptoms, doctors are asked to rely on subjective findings. Subjective findings are the bane of our lives. Don’t even get me started on the pain scale.
One specialist and I spent months experimenting, testing, endoscopies, and biopsies, trying to find a good marker for me so we could see if any treatments were helping. All we ended up doing was almost killing me when we found out I was super allergic to the multiple feeding tube formulas I was briefly on. That was SUPER helpful to know, so I count the whole thing as a win (no other circumstances would have given us the allergy info). But my doctor still, years later, feels horrible about making me so sick–and that it still didn’t even give us an accurate, objective way to measure anything objectively on me.
I’ve had doctors that won’t give weight to subjective findings. If there’s nothing clinically wrong, then there’s nothing subjectively wrong–the patient is either making them up or exaggerating them. I worry that the ordering doctor will review the results whenever I get a normal lab result and say, “Ah, just as I thought. Megan, you’re fine. You’re just malingering. You need to lose weight and exercise. Here’s a psych referral.” Or they might even note in my chart the terrifying label of “Munchausen’s.” I think this is something most, if not all, patients with invisible diseases are terrified of. Especially those with the really invisible diseases–the conditions invisible to even lab tests.
Doing My Part in the Process
Fortunately (?) I do have a few physical symptoms. Anaphylaxis is obviously a clear, objective finding. But even my hives are mostly invisible! How the heck am I supposed to show doctors I have hives when they are under my skin? Before I had my significant symptoms, I had years of a lot of little problems with very few supporting clinical findings.
I’m so incredibly blessed to have doctors who believe me. They keep looking and running test after test, trying to find something they can measure. And when we don’t see anything, they still listen, and they still believe me and my symptoms and still keep treating me. I’ve worked hard to be a trustworthy patient, so what I describe is accurate and not exaggerated. I keep notes and journal my health so I can be a reliable witness to the failings of my body. I work hard to be an active and educated participant in my health journey. If I am not, who else will be?
I know how often doctors cannot trust patients. As Dr. House so often said, “Patients lie.” I earnestly seek to be the patient who does not.
How else will the doctors believe me when it’s my labs that are the ones lying?
Did you know you can have epilepsy for decades and not know it? Turns out that’s true. I am Exhibit A.
It started with a twitch. I have a neck twitch. Weirdly, my twitches are unrelated to my epilepsy and they have now been diagnosed as something else–despite that being the family joke for years. But the twitches put me on the path to the epilepsy diagnosis. And in true ✨️Megan Fashion✨️ I did it backwards from most patients. Sigh. Haha.
I’ve been in a specialized type of physical therapy (PT) for my dizziness (at least that’s what it started for), and extreme fatigue, and I’ve found out there are other issues through this PT. It’s been so incredibly helpful.
I LOVE my physical therapist. She is one of the most helpful and open-minded providers I’ve ever had. She’s listened (and listened and listened, lol) to my various complaints and has helped me find the right avenues to figure out what is wrong whenever something new pops up. And I like to think we’ve bonded over our neurodivergent brains. hahaha
In an appointment in the Spring of 2023, I mentioned that one of my exercises was particularly triggering to my twitch and my PT doctor was confused. “What twitch?” she asked. I was confused. How did she not know about my twitch? I’d been coming for almost two years. How had she not noticed it? I twitch many times a day. And I ask most doctors about it…or at least mention it to them. So she asked about my twitch at that appointment.
No, I don’t lose consciousness. It’s usually in my neck, but sometimes in my face and/or arms, or legs. Usually on the left, but occasionally on the right. The twitches happen more often when I’m tired. And talking about it makes it worse. Just talking about it made it happen a bunch in that few minutes. I get quite embarrassed when it happens a bunch of times in a row and I know someone sees it. It’s usually a quick motion of my head, so it’s not always seen, but sometimes it’s repeated several times in a row, which can be annoying. Fortunately, it doesn’t hurt.
My PT asked if anyone had ever identified it, or if I’d seen anyone about it. Yes, I’ve asked multiple doctors (I’ve lost count, I usually mention it when I think it might be relevant) and no, no one has ever had an answer. She asked a few more clarifying questions and smiled slowly.
My Twitch has a First Name…
“I think I know what it is.” She went on to describe the condition, which mirrored my experience. She said it’s essentially a software issue with my brain, rather than a hardware issue (like a brain tumor or MS would be). It’s a legitimate neurological condition. I’m not crazy. And it’s real. But what was the name?! I was dying to know there was a name for what it was. She finally said, “Functional Neurological Disorder.” (FND)
Well, that’s the lamest and most unidentifying name ever,” I laughed. But I also felt the cool relief run through me that there was a legitimate name for what the twitch was.
A Series of Fortunate Doctor Appointments
My PT suggested that I see a specific neurologist at my hospital, who is an expert in the condition and could be the one to diagnose me. Perfect! I sent a message to my Primary Care doctor (she’s also wonderful) and asked her to make the referral.
A few weeks later, I had the ovarian cyst issue. Fortunately, I had a follow-up appointment with my Primary Care doctor a week later that July, so I reminded her about the referral request, which she sent in during my appointment. When I followed up with the Movement Disorder clinic where this doctor is, they said it would be nine months if I was lucky. Sigh. But then a few months later, I was lucky enough to get a cancellation and my appointment was scheduled for November.
I included all this about the timing to just show how long it is to be in limbo. How long it takes to go from appointment to appointment. It’s mentally exhausting, for sure. And I have it easy. I have excellent insurance that is generally willing to approve visits and tests, and (if I pay for the premium plan) a wider range of doctors on my insurance’s authorized list. I’m jumping ahead a little, but it’ll be just over a full year from that first conversation about my twitch with my PT to when I’ll get the week-long EEG done for epilepsy testing. A YEAR. What in the SAM HILL is happening here–that it takes a year to confirm epilepsy from the first conversation with a provider. Anyway, I digress. [clumsily climbs off soap box]
The FND Doctor Appointment
In November 2023, I met with this new neurologist, who was as great as my PT said she would be. 🙂 She confirmed the FND diagnosis, so that was nice to finally have an answer for my twitches.
In questioning me about my twitches, she asked me if I ever had audio hallucinations. I said no. But I thought of times when I had smelled things that hadn’t actually existed. So I told her about that. “Olfactory Hallucinations” turns out are a thing. So that’s fun. Guess I’ve been having them since probably high school? Maybe longer? I smell raw chicken, or raw pumpkin (both smells I hate and make me nauseous), or smoke–like electrical smoke or wood smoke. None of the smells happen at the same time. She asked me about the last time this happened.
The last time this had happened had been about 6-8 weeks before. My roommate and I were both home and I thought I smelled electrical smoke. I felt very anxious and compelled to find the source. I wandered around the house smelling for it but found nothing. My roommate and I both checked around the house and neither of us could find anything. I kept smelling it, but couldn’t source it. My roommate smelled nothing at all. It was stressful for me! What if there was a fire in the walls and we couldn’t find it!! Deep breaths. I remembered the whole thing, still do, and there was no blacking out.
These instances don’t happen very often. But I remembered this was not the first time I’ve thought I smelled smoke in my house when nothing was burning and been super anxious there was a fire in the walls–and there wasn’t. It’s happened multiple times in my life.
Another Referral
After I explained this instance, the doctor said she wanted to refer me to the seizure clinic just to make sure I was not having seizures. She said it’s possible that these instances are part of migraines, but they might also be seizures, so we need to make sure they weren’t. She made the referrals to the Seizure Clinic, a brain MRI, and an EEG to test for seizures.
I was flabbergasted. Was it possible I was having a seizure and didn’t know it? Was that a thing in epilepsy? I knew of only two kinds of epilepsy: petit mal and grand mal seizures. And I wasn’t losing time, so I didn’t think I was having those. I wrote it off as an overly cautious doctor and agreed to go. BUT I would rather have an overly cautious doctor who ordered tests and made referrals than a doctor who ignored things I was concerned about. I’ve been wrong about so many things about my body that turned out to be symptoms. Clearly, I don’t know anything about my body. Haha!
More Testing
In January 2024, I had the MRI (which was a whole thing), and the EEG. The neurologist messaged me after both and noted that they both came back clear with no abnormalities noted. Wonderful! I wasn’t having seizures! Or at least the tests didn’t catch any… I felt confident that the one thing I didn’t have to worry about now was seizures. We can move on. Yay!
I came so close to canceling my appointment with the Chief of the Seizure Clinic. I was absolutely convinced he was going to say I’m not having seizures. Why put myself through another appointment where another doctor was going to shrug their shoulders, at best, and say, “That’s weird, not sure why that’s happening,” and send me on my way. At worst, I’d get the “you’re wasting my time” brush off almost immediately and the doctor wouldn’t even spend any time on me if they didn’t believe me, or try to gaslight me into convincing me I’m wrong. I’ve seen all of these kinds of doctors through the years. Sigh. My chronic illness patient friends will know all about these kinds of doctors. They know doctors like my PT doctor, my primary doctor, and my FND neurologist are rare unicorns. 💜
The Seizure Clinic Appointment
So I walked into the appointment fully, 100% expecting to hear, “Congrats! No epilepsy! and Goodbye!” Instead what happened was interesting and better, and kinda worse.
The doctor did a full neuro workup (awesome!), asked me my history, and asked me about the symptoms that had me referred there. I was very grateful he took this seriously despite my clear tests. I wasn’t getting the brush off! With a bit of relief, I went through them again. I remembered, that I occasionally had auditory hallucinations–where I’ll hear music I almost recognize or remember, or can sing/hum the lyrics but can’t quite remember. I let him know about that too.
After we went through all this, the doctor sat back, “Well, I do think you’re having seizures.”
I’m sorry, “WHAT?!”
I’m not sure I’ve ever had a more clear jaw-dropping moment in my life than that one to this point. Like comically so. It would have been hilarious to watch from the outside.
“Yes, your symptoms are consistent with epilepsy.”
I was reeling. “But my tests were clear…”
“That happens sometimes. That just means you didn’t have a seizure while the tests were happening.”
“I’m sorry, can you clarify? Are you diagnosing me with epilepsy?”
“Yes.”
I blinked and blinked and blinked. What was I supposed to do with this information? I still don’t really know what to do with this diagnosis, even now weeks later.
Part of the reason my headaches have been getting worse over the years was because of the seizures (very helpful to know, lol!). He said that one of my meds is also conveniently an anti-seizure medication, so he upped my dose. He said that the reason I’ve had fewer seizures in the past few years is likely because I started the medication and we had been slowly increasing the dose.
The doctor also said that he wants me monitored for a week in the hospital on an EEG to confirm the epilepsy diagnosis. A week in the hospital! I could still work from the hospital, so that’s good. It would be another 3-4 months out. sigh. (Spoiler–it ended up being a 5-month wait–and over my birthday, so that’ll be…fun. lol) I’m not looking forward to this and I’ll be bored. But as my mom said, I’ll get to stay at a 5-star “hotel” with all my meals catered and room service for my birthday! I’ll be waited on by my own personal wait staff (love you nurses and CNAs!!). And I like the hospital’s creme brûlée, so it’ll work out. 🙂
Still shocked, I couldn’t think of any questions except: could I keep my license? I had been worried about this. Fortunately, the doctor said I could, since I don’t lose consciousness. WHEW. Such a relief.
I was sure there was a ton of information I needed, but it was subtly clear the doctor was anxious to get out of there, so I didn’t ask any more questions. After the nurse came in and handed me my check-out paperwork (“Don’t call us, we’ll call you to schedule a follow-up”, uh, okay?) I realized I didn’t even know what kind of seizures I was having. I was so overwhelmed and confused.
What Now?
It would have been nice if the doctor or nurse had provided me with resources or even pointed me in the direction to get more information. Fortunately, I’ve been diagnosed with enough conditions that I know how to do medical research and how to find reliable resources. But in that moment, it would have been nice to have something in my hand and someone knowledgeable to talk to. Anyway. So I did the next best thing: I called my resident on-call nurse.
I called my mom. I think she was more shocked than I was. Can’t imagine why. How do you miss that your kid is having seizures?? lol. To be fair, I never told her about the very weird olfactory and auditory hallucinations. When I was a kid I wasn’t quite sure they actually were happening so I usually just brushed it off, in my defense. They were short and did not happen together or super often. I just always thought they were a weird “Megan Quirk”™ and I had so many “quirks” (which were, surprise, symptoms of all my different conditions) so why bring up another one for a doctor to shrug or roll their eyes at.
Turns out that hallucinations were one that I should have mentioned. OH WELL. hahahaha. And in researching epilepsy since then, I’ve had some other symptoms since childhood too, like a lot of deja-vus, near-constant and worsening headaches, and apparently seizures that have auras with my other senses.
Congratulations on Making it to the End
I found out from my doctor’s chart note that I have focal aware and focal absence seizures (probably because they are probably happening in my sleep too–sometimes a smell or a loud noise has woken me up). These are the most common types of epilepsy–I’ve learned this from researching epilepsy on my own.
So remember days ago at the beginning of this post when I said that I go about things backwards? Usually, people go in for seizures and walk out with an FND diagnosis. Well, I walked in for an FND diagnosis and walked out with an FND AND an epilepsy diagnosis. #onbrand
There you have it. I have epilepsy. Fortunately, it seems fairly well controlled (I think??) and doesn’t seem to really impact me much. If you see me panicking over the smell of raw pumpkin and it’s March–just tell me to chill out and it’ll pass in a minute or two. It’s just a little seizure. 😀
If it’s October–well that’s just (probably) because I hate the smell!
Disclaimer: I’m not a doctor and this is not a way to be diagnosed. 🙂 If you think you are having symptoms that sound similar, please find a doctor who will listen to you and take you seriously. You are your own best advocate. 💜
I’m currently in my 18th hour of an ER visit. Hour 24 without food, and hour 30 without sleep. And the right side of my abdomen is currently being stabbed with a pitchfork every time I move or breathe, and every other time I blink. Actually, they gave me pain meds a bit ago again so it’s down from a 9/10 on the practically meaningless pain scale to a manageable (and my pretty standard operating condition level) 5. So I’ve got that going. I also have iv benadryl (and it feeeeellllsss soooo goooood!) and my safe steroids on board too. So if this is incoherent, we’ll blame it on that, m’kay?
Disclaimers 🙂
So first a couple of disclaimers before telling this story:
1) I know I’m incredibly blessed and privileged to have access to great health insurance and a world-class university hospital that is willing to recognize my many, weird diagnoses and treat me. So many with my conditions go without this and it’s absolutely heartbreaking.
2) I’ve had some rough ER visits that leave me worse off than when I walked in, so it makes me quite gun-shy about going into the ER. I’ve skipped going in because the stress of having to defend my needs sometimes outweighs what is potentially emergency room worthy. I’ve learned to (mostly) diplomatically advocate what I know my body needs and respect the doctor and their experience, and who are likely inexperienced with my constellation of conditions. It’s a tough needle to thread. Sometimes doctors don’t respond well to me defending what I need or trying to explain my prior experiences.
I’ve talked before about what getting my bingo card (my current favorite analogy) collection of unusual and rare conditions looks like. But other than those fun adventures, I haven’t had many other “normal” issues. If you ignore all my problems, I’m like *totally* healthy. Haaa.
An ER Visit Personal Record is Broken
But yesterday, I had a normal person health problem that ended my 4.5-year no E.R. visit streak. (Can I get a round of applause for that streak?! It’s dang impressive for me!) Mid-afternoon I started having severe pain on the right side of my abdomen. It was low and it was terrible. I tried my usual bag of tricks thinking it was related to my usual suspects. But instead, I felt worse and continued to get worse. A consult was made with my local access, on-call nurse (thanks for picking up mom!) and I was advised to go to the ER. I bet you can guess what the concern is here. Lol.
I went to my hospital at about 7:30 and it was PACKED. I was in so much pain I could barely shuffle to the check-in window. There were no wheelchairs (spoiler alert: none for hours). I checked in and shuffled down the hall to find a chair. Luckily, someone was called back right then so I hobbled at a glacial pace to the chair. Triage got me about 20 minutes later, took labs, and noted my symptoms.
This photo was taken long after most people had either left because of the long ER wait or had been taken back to a bed. Finally, a wheelchair is available. I didn’t get to use it.
Tales from the Waiting Room
Over the hours, my pain was getting worse. There was a guy who came in a couple of hours after me and appeared to be in significant pain. His approach to getting quicker help was to gradually get louder and eventually got to yelling his discomfort and so he got wheeled back hours before I did. Sometimes suffering in silence is not helpful.
A hilarious interaction I saw was between two men in their 50-60s who were swapping stories. They were sitting next to each other and said they had both been waiting most of the day. They showed each other their left legs where they apparently had both received bug bites of some kind (they guessed spiders). Their budding bromance continued as they watched Jumanji on the waiting room tv together. It made me giggle.
You know, there was something oddly comforting sitting there with other suffering people, knowing I wasn’t alone in my pain and frustration at the long wait.
(So about 7 hours after arrival) I was taken back to a bed and had a chance to finally meet with a doctor.
I just got called back for my CT scan (second attempt) so hopefully they’ll do it this time. I’ll finish writing this later. Please hold.
A Long Story Gets Longer
Okay, I’m home from my ER visit. I was there for 23 hours, and awake for 38 hours (DO NOT RECOMMEND, lol, also might be a personal record?). Oh, man. But we know what happened and what happens from here. And my MCAS reactions were managed quite well. Overall, I’m happy with how it went. Definitely one of my better ER visits. So here’s the rest of the story.
Around 3:30am, on a crazy busy night, I finally made it to a bed. I was utterly exhausted and nervous about how I would be treated by the doctor. Surely they were also having a tough night too.
The CNA wheeled me back into a pretty private area. There was only one other bed in the bay and they were separated by a hard wall. Other bays were open and had 4-6 beds and were much more chaotic. So grateful for where they put me. It was quiet and they kept the light in my “room” off. I don’t like overhead lights. My night nurse, Melissa, came right in. She was wonderful. I explained what was going on and a bit of my prior medical history. While we were going through it the doctor came in. Dr. Tim. Never had an ER doctor introduce himself with just his first name. Haha. He was so great!
We Make A Plan
I went through everything again and Dr. Tim said he thought I need an ultrasound and a CT. He thought I might have a torsion of my right ovary (where the intense pain was) or possibly appendicitis. He also noted that I had some pain up higher on the right side of my abdomen that seemed to be different than the lower right pain. Basically, all of my right side was painful. We discussed pain meds and my allergies to find one that would work for me. I don’t like narcotics and have had reactions to a few of them. We settled on Norco starting at the lowest dose and would work up if I needed it. Fortunately, 5mg of Norco every few hours was enough to cut my pain from 9/10 to a 5. I could handle that.
Dr. Tim left to get the orders in for radiology. Melissa confirmed my triage labs didn’t indicate an infection, and that I wasn’t pregnant (oh good, my pains were not from labor! Whew! hahaha), but because of my primary immunodeficiency, we needed the CT with contrast to confirm. I hadn’t realized the CT was with contrast, so I immediately said that I was allergic to contrast. So now we had to make a plan for how to get the imaging we needed. Dr. Tim discovered the allergy at about the same time and came back a few minutes later to discuss it.
We talked about my previous reaction. My previous premed protocol was 13 hours: oral dexamethasone (dex) and benadryl the night before and IV dex and benadryl the day of. But I reacted on that, so I needed a better pre-med protocol. And preferably one that was not 13 hours long. Dr. Tim thought we could get away with a 5-hour one if we did higher doses of meds. I’d have my ultrasound in the meantime. I didn’t know if 5 hours was enough, but I was willing to try. With a protocol like this, timing is super important so I needed to get meds at the right times and get the CT at a certain time when the meds are at their peaks.
I got my IV with an ultrasound tech. It was so easy. The girl got it on the first shot. Yay! I prefer IVs in my hands, but CT with contrast requires it in the forearm or higher. But it’s usually difficult to get it anywhere else. Historically, it has taken up to 3-4 or more attempts, even in my “reliable” hands. I have lame veins that like to fight off the invading force of the IV. But this was a breeze. Ultrasound placement is the way to go!
Yay for easy IV insertions! And glowy ET fingers!
Ultrasound Time!
Around 6:15am I went for my ultrasound. And I found out I needed an external and the dreaded internal ultrasound. I was not excited. Because the Ultrasound Tech was a guy, the EMT that wheeled me over stayed for the scan and the three of us had an interesting conversation about her decision to go to nursing school. Which was a good distraction from the internal ultrasound. The Tech was a bit of a jaded medical professional (definitely still professional, and honestly, I can’t blame him), but the sweet EMT was excited to be a nurse. I’m rooting for her and told her that I was grateful that there were still people who wanted to be nurses in a post-covid world. And as an EMT working in a hospital, she clearly knew what she was getting herself into. I see good things for her. 🙂
By the time my ultrasound was done, shift change had already happened. When I went back to my room, I met my new nurse, Lucas. He was good, just not as friendly as my previous nurse. I like to get on good terms with my nurses, but he was a nut that I wasn’t quite able to crack. He did his job but wasn’t interested in learning about my conditions or spending time talking. That’s totally fine. But I always appreciate it when I meet medical professionals who want to learn about them.
CT Drama
Four hours after I got my dex, I went to CT. I let them know about my prior history and they then pow-wowed about what to do. One of the techs was sooo kind. He could tell I was nervous and spent time with me making sure I knew they were taking my concerns seriously. I had been so cold in the waiting room and hadn’t had a blanket, unlike everyone else. So the tech went and brought me all the blankets and bundled me up. Hahaha. It was very sweet. I warmed up quite nicely in the chilly CT room.
The other tech and the radiologist came back and let me know I needed a longer premed protocol (I knew I would) and they were sending me back to my room. I didn’t want to be in the ER longer than I needed to be, but I knew I needed more meds before getting a CT with contrast.
Waiting for everyone to finish their pow-wow and to be inevitably sent back to my room without my CT.
A New-ish Plan
I made it back to my room and finally met my day doctor, Dr. Megan. She was also so great! By the time she came in to see me, she’d talked to Radiology and looked at my chart. She had me recap what brought me in and my general MCAS history so she knew what she was dealing with.
She let me know that the ultrasound found a burst cyst on my ovary, but no torsion so I didn’t need emergency surgery on my ovary. What a relief! I also found out I have gallstones. That explained the pain in the upper right part of my abdomen. She said the ultrasound couldn’t quite tell if there was a current infection, and the CT would give us more information about my appendix and gallbladder. She wanted to check with Pharmacy and Radiology and come up with a good pre-med plan.
A bit later she came back and let me know that they had found a new pre-med plan that was stronger and shorter–only 9 hours, and they wanted to go for it. She also said there will be a doctor in the room to make sure I got epinephrine if I do react. I was all for not being there for a shorter amount of time. And a liter of fluids after to help start flushing the contrast out of my body. I got my second shot of dex. I felt good about the new plan.
CT Takes 2 and 3
About 2:30, an hour before my CT, I got my last dose of dex and benadryl. At 3:30pm, Radiology was gifted with my presence again. The swing shift had replaced the morning shift and missed the memo about my situation and high maintenance-ness, so almost immediately I went back to my room. If we couldn’t get this handled quickly, it was going to be another 4 hours (and another shift change) because of the medication timings.
Fortunately, my doctor was able to work it out quickly and I went back to CT within 10 minutes. I had the same tech as the morning and she remembered me, so that was comforting. My nurse came with me and confirmed he would give me epi if I needed it, so that was also comforting. He also brought oxygen, which turned out to be a good thing.
The radiologist wasn’t super patient with me and didn’t really want to listen. He kept saying that I was pre-medicated so I won’t react. I couldn’t tell if he meant to reassure me or tell me I was wrong about my body. It came across as the latter. I told him I was premedicated last time and still reacted. It didn’t seem like he believed me. “I’ve never seen someone react when they’ve been pre-medicated.” I decided to respond with “Let’s hope your record remains unbroken,” instead of, “You’re about to see the first.” I was as prepped as I could be.
And…I did react…but not as bad as the first time, and not as long. The supplemental oxygen helped me feel like I could catch my breath faster, so that was helpful too. I didn’t need any epi. So mostly a win. I mean, I survived, so really, it was a full win.
An ER Visit Comes to an End
Back in my room, I started my fluids. My nurse said it would take a couple of hours to get the CT results. However, my results came back in like 45 minutes. (I think the radiologist just wanted to get rid of me, hahaha!)
Dr. Megan came in and let me know I had no appendicitis! I did not need any emergency surgeries! Woohoo! And I could have food and water again!! Best news of the day.
But she said I needed my gallbladder out because of my gallstones. They’ll only bring me trouble and will possibly cause an infection down the road, which would be very bad. The nice thing is I have time to plan this out and make arrangements for the surgery and save up for the time off. And I will have time to find a surgeon and anaesthesiology to make sure we all feel comfortable. Which is a huge relief.
She also let me know that it looks like when my ovarian cyst burst, it messed up the placement of my IUD so I need to get that replaced ASAP so it doesn’t damage my uterus. I just replaced my IUD a couple of months ago. I’m not excited to go through that again. Ugh.
And as a nice bonus, it turns out my ER doctor is friends with my primary doctor. So Dr. Megan said she’d call her right away and catch her up. I’m very grateful. Conveniently I have an appointment with my primary doctor next week for something else, so we can also talk about my gallbladder, and make sure I’m still doing okay, Another small blessing in the timing of this. I also already have an appointment with a new gynecologist in a few weeks and I can hopefully get my new IUD then, which is also convenient. And as a parting gift, Dr. Megan said she documented the pre-med protocol in my chart so if I ever need a CT with contrast, we can use it again since it worked so well. So grateful!
An Almond Sized Cyst
Without my 3.4cm cyst, I would have never known about my gallbladder. So while quite painful, it saved me a potentially much bigger problem, and for that, I am very grateful.
As soon as my fluids were finished, Lucas pulled my IV, and I was officially discharged! What a relief! I had to wait a bit for my pain medication prescription, so I went to the cafeteria for a light meal to ease my stomach back into food. It had been 28 hours since I had eaten. I can’t fast, so I was a bit nervous to eat. A lot of water, a bag of salty chips, and a bowl of honeydew later, I was feeling pretty good. I picked up my meds and busted out of the clink! My ER visit was over! After 23 hours, I was as FREEEE as Dobby (you know, before he bit the dust, poor Dobby)!
Let me just tell you, after a long, cool shower, and sleeping 13 hours, I feel like a new woman. I still have some pain, but I can deal with it just fine.
A Good Doctor Makes All the Difference
I just want to end this by noting what a difference it makes to have medical providers who are open-minded and good listeners. It is really nice when they recognize patients who have complex and rare medical conditions are the experts in their own conditions. Both of my doctors specifically said, “You are the expert in your condition. So you tell me if ___ won’t work and let’s figure out a solution so you feel as safe as possible.” It was such a different experience this ER visit than even the last time I was in the same emergency room. I had a different doctor who never even told me her name and got frustrated that I couldn’t communicate well (because I was having anaphylaxis?!).
I know doctors are people too, and everyone has rough days at work, and ERs are especially stressful. But bad or even impatient doctors can be traumatizing to have in a crisis when you don’t have a choice about who you see. I don’t have family who live near me. So I’m always alone at appointments and in the hospital. That is stressful. However, good, compassionate, open-minded medical professionals make such a world of difference to the “professionally” sick (and really, all patients). And I am so, so grateful for them. Maybe, just maybe, I won’t be so nervous to head to the ER next time I might need to.
I’m so grateful I learned some new things (like some of my meds can cause significant side effects to my heart, which I didn’t know about so now I can stay on top of monitoring for it!). I got a new protocol in my toolbelt, and walked out better off than I hobbled in.
So now my right side is looking sunny side up!
An Egg Sunny Side Up. Ironic since an unreleased egg is what caused all this ER visit drama. hahaha. Image by maddas from Pixabay